Steve Maleham and Helen Simmonds of PCC discuss the latest toolkit for primary care networks
Steve Maleham, associate, PCC
Helen Simmonds, adviser, PCC
During mid-November 2021 we saw the launch of the latest toolkit to support primary care. It was designed to support primary care networks (PCNs) with their estate planning and development of estates strategies. More and more practices and PCNs are now starting to develop their estate strategies as staff numbers increase due to the additional role recruitment scheme.
The toolkit has been developed jointly by Community Health Partnerships (CHP) and the National Association of Primary Care. It has been developed to provide a national framework that will support PCNs and integrated care systems (ICSs) to identify their primary care estate change and investment requirements whilst facilitating consistency, and supporting service development strategies, across the wider health economy.
It’s really important practices engage with the service development and estate strategy that their PCNs are developing to ensure that each practice’s future aspirations are considered. The new toolkit builds on the guidance publication Primary Care Networks: Critical thinking in developing an estate strategy which was published in March 2020. The toolkit has two objectives:
To enable each PCN to identify and prioritise their estate optimisation, disinvestment, and subsequent capital investment requirements to address population health priorities and future service needs.
To support the production of capital investment plans for PCNs and places and help ICSs to aggregate and prioritise local primary care investment requirements against other system demands for capital.
So, what does it contain and how should we use this?
The first thing to say it that is not mandatory; PCNs are not obliged to use the template, so if work has already started in your local area, you don’t have to start again. However, the toolkit has been designed to utilise data and analysis already gathered via the primary care data-gathering programme (PCDG) and live local datasets held on the SHAPE PCDG Atlas. Each PCN will be able to request a pre-populated version of the templates, with their local SHAPE data embedded, in order to provide a good starting point
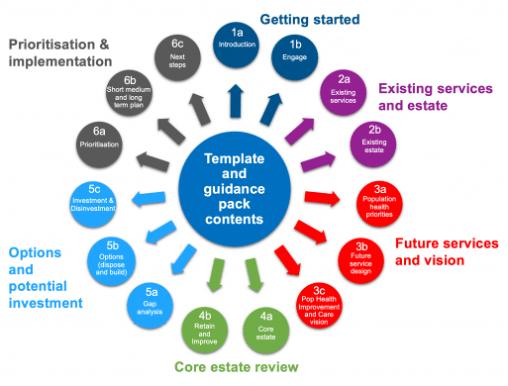
The toolkit contains a PowerPoint template which contains all the sheets to populate and links to external excel templates which can be pre-populated at PCN level, based on the data available, and then developed and updated. Each section has a supporting guidance document to help people understand what to think about and how to populate. It also suggests running some workshops and gives you the topics to be covered, etc. The outcome at the end of the process is a robust, evidence-based PCN service and estate investment plan, supported by a population health-led clinical vision, based on current PCN estates information.
Fig 1: The contents of the toolkit
The toolkit will help each PCN to fully assess its existing estate against its local clinical vision, service strategy and forecasted demand. It is envisaged that every building will be able to be placed into one of the following three categories:
CORE – buildings that will remain in operation delivering primary care services for at least the next 10 years.
FLEX – buildings that will be providing primary care services for at least the next five years but may not be needed longer-term as the clinical model evolves.
TAIL – buildings that are likely to be disposed of within the next five years.
In addition, following the processes set out in the toolkit will enable PCNs and local health systems to identify how much investment is required, with each building placed into one of the following classifications:
Category F1 – building is surplus to requirements and will be disposed of within the next two years.
Category F2 – building is in urgent need of a minor improvement grant (MIG) within the next two years for it to meet all Care Quality Commission and statutory legal requirements. This is an investment that must be made for building compliance reasons irrespective of the clinical model if the building is to remain operational.
Category F3 – building is likely to be surplus to requirements and can be disposed of within five years if appropriate investment is secured for alternative and replacement facilities.
Category F4 – building will continue to be core operational estate and will require only a small amount of investment of less than £250,000 between years 3-5. Buildings in this category are likely to be candidates for future MIGs.
Category F5 – building will continue to be core operational estate over the next five-to-ten years but will need significant investment (£250,000-£1m) in order to meet demand growth and/or changes to clinical strategy. This could be a building extension or a significant refurbishment/ reconfiguration.
Category F6 – these are options where new facilities are likely to be required over the next five-to-ten years. These may be new buildings but could also involve the re-purposing of existing buildings, such as retail units, or include moving into existing NHS estate, such as community hospitals or CHP LIFT/NHS Property Services buildings.
Access to the toolkit is freely available via a simple registration process which enables the download of the generic templates and guidance notes from https://shapeatlas.net/pcntoolkit/
Access to pre-populated templates for a specific PCN requires the applicant to confirm consent that the GPs within that PCN are happy to share the data. For support and queries, please contact [email protected]
If you are looking for support to develop your estate strategy our team of premises advisers are able to assist. Contact [email protected] to see how we can help.






Be the first to comment